

An Immunologists' Personal Decisions On Mask Wearing In 2026
How I have updated my thinking going forward while SARS-CoV-2 is still present, and what would change my mind again.

Introduction
I am and always have been an incredibly COVID-cautious person. I have worn a mask consistently in public except for a very rare occasion since 2020. I am still “COVID 0” meaning I have never acquired SARS-CoV-2 to the best of my knowledge. This is backed up by rigorous testing performed on me and all household contacts (we were all negative) the three (3) times I have been sick since 2020. It has been fantastic to not get sick while traveling (I travel at least 10-20 times a year for work) and to spend my holidays completely healthy. I will therefore always mask in several of the situations described below. However, this last year I have relaxed my masking due to changes in data as our population, the world is adjusting to endemic SARS-CoV-2. Therefore, as a long-time advocate for mask wearing, I thought it would be helpful for people to understand how and why I have made the decision to relax my mask wearing strategy.
There are some important disclaimers for this post:
First, as it always should be for everyone, my personal health decisions reflect my personal risk tolerance. This risk tolerance can and will change if I or a family member need extra protection from pathogens in circulation. I encourage everyone to take their own personal risk assessment seriously, do your homework, talk to your doctor, and to protect any family members and loved ones that may be vulnerable.
Second, I am rarely exposed to large groups of people and when I do I am selective and thoughtful about when I wear a mask and when I don’t. I don’t work with any vulnerable populations, or the public. Lower rates of interaction mean that I inherently have lower overall risk of virus exposure in any given year. The team I do work with is encouraged to work from home or take a day off when sick, and if someone does come in mask wearing is encouraged if they were recently ill. We also have access to excellent high turn over HEPA air filtration in all spaces.
Third, this review of my changes in personal mask wearing is meant to be educational and is not medical advice or meant to encourage a change in what you are or are not comfortable in doing. I fully advocate for anyone choosing to wear a mask at any time, or all of the time, and believe that this should be integrated by society and normalized. The world will be a healthier place if we can reduce viral infections.
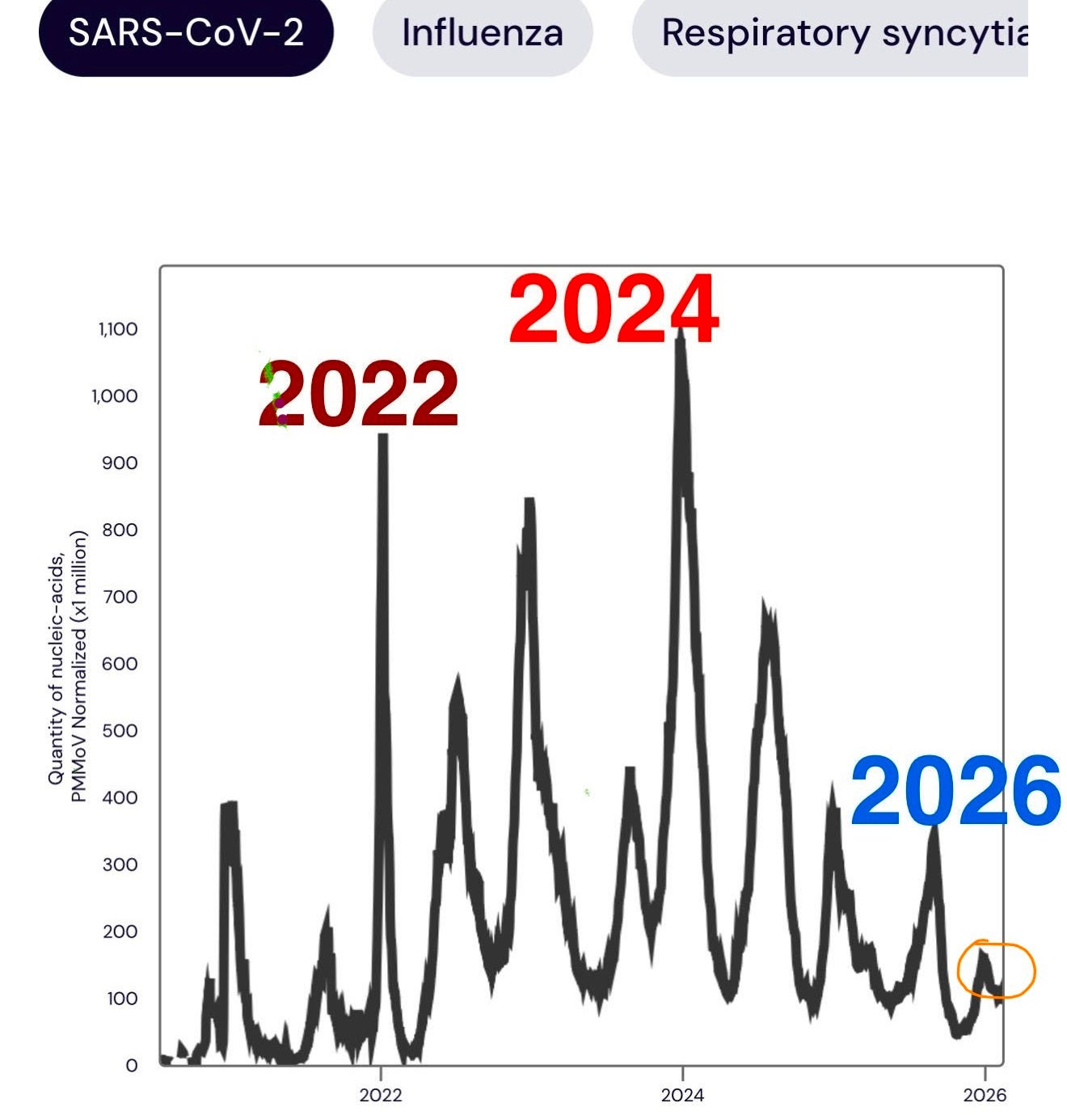
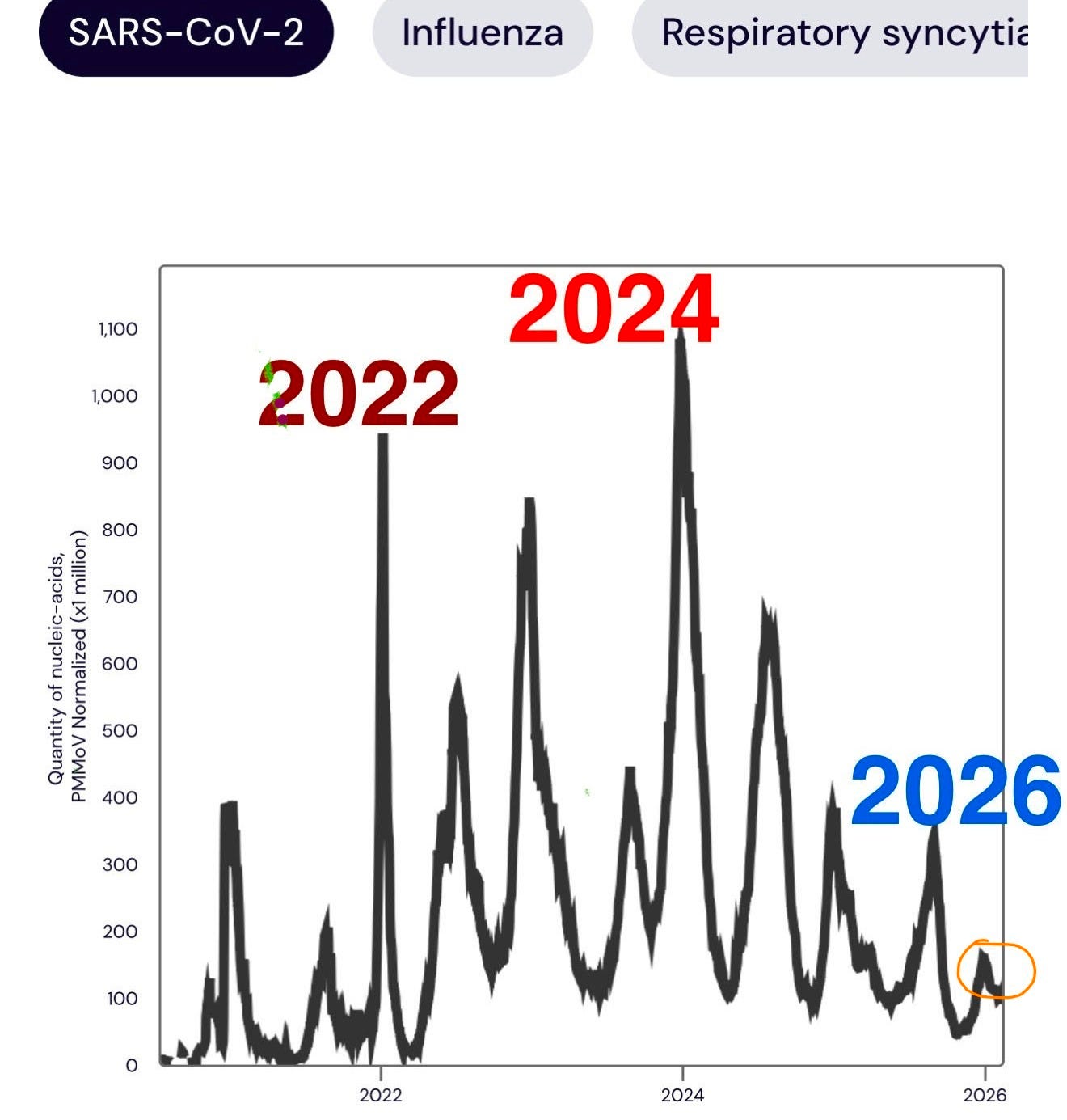
Fourth, my choices will change as new data is found/reported/generated. This is the nature of science and science based decision making, changes do occur. For example, we have now had a long period of SARS-CoV-2 virus mutations that has failed to fully evade vaccine protection in a way that lead to disease spikes like those seen in 2022 or 2024. In fact, this winter (2025-26) showed waste water levels lower than that of the summer, using the same methodologies and tracking stations across the United States (see below, circled in orange: source data WASTEWATERSCAN.ORG). But if a new variant that I am concerned about is identified, I will resume more careful habits and of course, let everyone know.
Finally, this post is not a call for ‘masks off.’ I am writing this post to communicate my approach to masking, that is specific to me. I don’t personally do well with unnecessary extremism in any direction, I find it difficult to maintain and something that on a societal level can cause knee-jerk reactions in the opposite direction. These thoughtless ‘knee jerk’ reactions and aversions to ‘being told what to do’ are something we are still suffering from as evidenced by low vaccine rates and the plummeting trust in scientists and doctors.
We did what we had to do during an emergency phase of the pandemic, and it certainly saved lives as there was no time for mass public education on complicated science that in many cases was still a moving target. But today, we are still suffering at the hands of the quacks that rode the counter-current of dissatisfaction to popularity and their anti-science rhetoric is verging on causing generational damage to our population’s health as well as science and medicine. Extremism has extreme results, often in unanticipated directions. I personally prefer educated and thoughtful approaches that are not extreme but are truly ‘doable’ and result in real, lasting change.
It is important to recognize that more or less risk tolerance often works on a ‘sliding scale’ for most people. This however can lead to decision fatigue so it is understandable that some people are simply mask off or mask on. Many people I’ve encountered online will never wear a mask and never have, some people have gone completely ‘mask off’ and used to wear one, others will never unmask in public again. Some people I encounter when out and about are well meaning, but still aren’t wearing masks correctly (well fitting, over the nose and mouth) and/or haven’t started using N95, KN95, or KF94s.
My greatest hope in starting this conversation is that it helps people who would like to stay healthy identify key situations where masking can help them to do so, and to encourage them to start to incorporate it into their daily routines without stigma. And I hope that others who feel ready to go maskless do so by confidently being able to think through what might be a high or a low risk situation.
Through this post I hope to educate people on how consider a multi-factorial risk landscape and adjust to it situationally. This is something that comes naturally to me having spent over 25 years working in laboratories where the things around me could kill me if I made a mistake. I’m still here.
I also recognize that few people reading this have spent decades in direct contact with or working around things that could end their lives or seriously disable them. So I understand the extreme aversion to any risk, especially if the risk is not well understood. Many people do drive a car and take that calculated risk daily, wearing seatbelts and observing the rules of the road. And while COVID-19 deaths have decreased, car crashes are still one of the leading causes of death. To paraphrase how I approach any risk: there are people who are old and those that are bold, but few that are old and bold. You’ll find a combination of caution, experience, education, and thoughtfulness and a ‘Swiss cheese model of protection’ is behind every one of my decisions explained below.
As with anything, risks are rarely zero but there are some times where they are extremely low and education is key to making informed personal decisions, and as always, discus any personal decisions and risks with your doctor.
Identifying Risks And How I Interpret Them
There is no magic equation for risk assessment, and all risk assessments are at best situational estimates. They aren’t perfect. Below I outline a few of the key ways I assess risk of infection for myself and how I might adjust my personal behavior.
Is the Virus Around?
For most of the pandemic, especially in the emergency phase it was easy to simply assume the SARS-CoV-2 virus was everywhere. On our groceries, in the air, and that every person could potentially be infectious. This of course wasn’t always true, but it was a quick hack to keeping yourself safe from what turned out to be an incredibly deadly and disabling virus. I ascribed to this thinking, and I know it is what kept me from getting COVID-19 to this day while some of my friends still suffer from lingering effects from the early variants. In reality, before mass vaccination roll-out, the peak of the 2020-21 infection season in January of 2021 only about 1 in 12 people who tested for SARS-CoV-2 were positive. That means every person who had a reason to test or what feeling sick only 1 of 12 were infected with SARS-CoV-2. Some areas have spiked higher, but typically peak global levels have been around 11% positive meaning of the people you’ve encountered out and about fewer than 1 in 10 (many people also do stay home when sick) would have tested positive for SARS-CoV-2 even at peak times of infection.
Studies examining asymptomatic infection find significantly lower positive rates among the general population when random testing of healthy people done a pooled asymptomatic infection rate across 29.7 million tests of 0.25% or 1 in 400 people (more about this later) was found. Furthermore, you can be in a non-infectious phase of illness, unable to infect anyone, and still be testing positive — though that long tail and how infectious people are is still debatable and may be situationally dependent. In general, most people are not contagious 5 days after their fever dissipates.
Going forward I have started to use local health department and wastewater data as an overall filter in my decision making. Wastewater science is a steady and relatively reliable leading indicator for infection rates. It will go up long before people start reaching for a COVID-19 test, and it doesn’t rely on people feeling sick and testing.
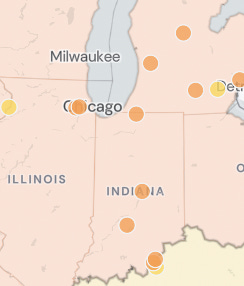
Here’s an example of how I might use wastewater data. This data is taken from wastewaterscan.org on February 16th, 2026. I often bounce between the San Francisco Bay Area and Chicago for work, but it looks like I should be more cautious about going out and about in the Chicagoland area right now, masking up more often due to the much higher rates of SARS-CoV-2 in the wastewater. The San Francisco Bay area and the Los Angeles area are relatively low, therefore, I would consider this in my overall decision making process. Because I like to stay healthy in general, I also typically scan through the other viruses tracked by this website and add those into my risk calculation.
In general, this winter has been very low nationally for SARS-CoV-2 in the wastewater, meaning fewer people were sick with this virus on average. How not to interpret this data is that the virus is gone or non-existent, it was still detected. This is simply an indicator that the chance of encountering someone who is infected with the virus will generally be lower in regions with lower wastewater levels.

Analysis of historical wastewater levels can also be helpful, revealing historical trends for virus peaks. For example, historically SARS-CoV-2 levels often start to rise after the 4th of July in the United States after which they have a summer peak, then begin to rise around the Thanksgiving Holiday peaking later in the respiratory virus season. That means these times might be good times to avoid getting infected as historically this is when rates of spread start to increase.
Overall I consider wastewater numbers and historical trends of virus infection when assessing situational risk. For example, during the peak wastewater spikes of 2022-2025 I would simply not go out to eat in a restaurant and was always masked in public. But during the early summer lull of 2025 when wastewater was low nationally, I did venture out into well ventilated spaces more often.
Any recent changes in the virus?
I check for new variants regularly. Because I am a scientist and have access to things like the GSAID database and have enjoyed tracking variant evolution tracking since first mutations were identified, this bit is always interesting to me. The average person however usually has to wait for a breaking news article and even then it can be difficult to tell if some of the headlines are real or clickbait. The wait then is even longer for a government agency to publish on the topic. This is where well researched social media creators have filled a critical communication gap, and I am proud to be part of that crew of people. In general if you’d like to wade into this science yourself you’ll be looking for a few key things:
1. How many mutations are in the receptor binding domain of the S protein? (This is SARS-CoV-2 specific, and if there are more this can mean it will be more immune evasive)
2. Do scientists indicate that it has vaccine evasion or is so significantly different from prior variants that it will be immune evasive?
3. Are there any indications that it has greater residence in the upper airways or high cell binding capacity? (this often correlates to a higher rate of spread)
4. Are there any indications of changes in symptomatic disease in people who are infected?
If there are changes in a variant that make it immune evasive this alone can be problematic, even if the disease is considered more '“mild”. This was what I still consider a significant error in the messaging about the Omicron variant. While it was less deadly on an individual basis, it killed far more people than the Delta variant due to it’s rapid rate of spread and immune evasion. This is one example of where social media rifts developed, some scientists chose to communicate how it was more mild, others continued to explain that this wasn’t well established and that it wouldn’t matter if it was still deadly and spread more effectively. I’m proud to say I got that one right and was in the later crew.
Once a new variant is identified, especially if it is found while people are ‘headed back inside’ for cold winter months, or that end of summer wave in the Northern Hampshire is starting this can mean that a new wave is coming or will be amplified by the new variant. This will shift my masking behavior towards being more often.
Most of us will get to avoid being in a city or town that is 0 for a new variant, so you will likely have a bit of prior notice and a few weeks to shift behaviors towards masking more often.
Recently, we have had a few new variants identified, there was a little immune escape from a variant this winter, but this failed to drive a significant wave of infection relative to prior years. I am keeping an eye on NB.1.8.1, however, I have not seen a pattern yet that is significant enough for me to sound the alarm to the public at large using my social media channels. This may change in the next week or two — just like any good scientist I follow the data.
When did I last get a vaccine?
We all know that vaccines are not magic bullets or silver shields, they fail, there are breakthrough infections. This is especially true when a vaccine only has one version of a virus (or representative protein), and 10 or more variants are in active circulation. The good news is that antigen exposed people (vaccinated, previously infected, or both) have immune systems that have been “educated”. T cells, for example, recognize the virus even if it’s not the exact same protein signature that was in the vaccine. Therefore, the immune evasion (changes in the virus) may allow the virus to get around the first line of defense of the immune system but it can quickly adapt to control virus replication and reduce symptoms, virus load, and impact of the disease.
At this point most of the world has been exposed to SARS-CoV-2 through infection, vaccination or a robust combination of both. Therefore, fewer people are getting very sick from the virus, fewer people are dying from the initial virus infection (data from countries around the world show this clearly), and fewer people are spreading the virus. It should be mentioned that disability from Long-COVID is still a significant risk from infection, but this too is reduced by vaccination, taking precautions such as mask wearing, and in many studies taking Paxlovid. Rates of infection, death and Long-COVID-19 can change if a highly immune evasive, deadly variant shows up, but this is where we find ourselves right now.
I still plan to and will continue to get an annual SARS-CoV-2 booster. Even though the antibody protection wanes (just like it does for influenza vaccines), the few months of protection it affords me in the winter months when infection rates are high is an important part of my ‘Swiss cheese model.’ This means that if mask wearing and situational awareness fail me, I at least have another line of defense onboard that can reduce chances of infection and severe outcomes. When the time comes and I am older or have good reason to (immunocompromised etc.) I will certainly opt for another SARS-CoV-2 booster mid-year.
Despite all of its detractors, the data is clear that the SARS-CoV-2 vaccine does reduce infection. Beyond that it reduces severity of disease which in turn reduces the likelihood of developing Long-COVID. But, about 3 months after getting my booster I do weigh that factor in my mask wearing choices, especially if SARS-CoV-2 is high were I am, and definitely if there is a new variant on the horizon. Remember this is all against the background of being a healthy, 40-something, who has no confounding health factors. If I did have additional health considerations, I would shift my masking to be more often.
What is the air circulation like, and is it crowded?
Now let’s talk about venue. Venue has quite a bit to do with rates of exposure and infection. Is the room you’re in is well ventilated with good air circulation and three-story high ceilings and are people well spread out (like a recent medical conference I spoke at)? Or are there low ceilings, you’re far away from any doors, and people are packed - something like a concert in the basement of a local dive bar that is at the fire code capacity.
One of these venues is clearly higher risk than the other. I also generally feel more comfortable unmasking outdoors or in event spaces that are massive with great air circulation. For example in a sports arena I may be unmasked for a brief period of time, but I will put on a mask when I visit the restroom or if someone feels too close or is actively coughing.
Airborne viruses can spread quickly in crowded spaces given the right circumstances. But it becomes more difficult when you’re trying to assess a local restaurant that is half-full. I try to err on the side of caution here. Often I choose to eat out at off-peak times. I’ll sit with my husband at the bar if no one else is there so we are away from the main crowded areas of the room.
Summer months are great because it’s always much safer to eat outside, that said if the person one table over keeps turning to sneeze in your direction — it could be allergies — but it could be something else. Taking into account the other risk factors discussed above is how I would shift my risk assessment of being in a building or eating out with friends. Is it a peak time for COVID-19? Is the local wastewater high? When was my last vaccine? Are there any new variants ramping up? If the wastewater is low, I have a recent vaccine on board and no new variants are up and coming, I feel more comfortable eating an uncrowded, well ventilated area. This doesn’t mean it’s completely safe, but it will be lower risk.
Hand washing
I tend to be a good hand washer. If you want to avoid viral infection, you should be too. Even before the SARS-CoV-2 pandemic I always had a bottle of hand sanitizer in the driver side door of my car (note: hand sanitizer does nothing for norovirus). The ever empirical scientist I am, I’ve done the n=1 experiment since my college years showing that when I routinely use it before grabbing a bite to eat or heading into the house after a day at work, I do not get sick as often. Some viruses live longer on surfaces than others, influenza A for example is infectious for much longer than SARS-CoV-2 is, but both can spread from fomites (inanimate objects that can transmit infectious disease).
Despite my good habits when I know a wave is coming or see a spike in the wastewater, I ramp up my handwashing alongside of my mask wearing. I also remind myself to avoid touching my eyes, nose, face or mouth until I’ve washed my hands. I’ll also wipe down personal items I routinely touch more often, including phone, laptop keyboard, glasses, and car steering wheel.
Friends, Family, and Other Close Contacts
I am lucky to have friends and family that respect that I don’t want to get sick with SARS-CoV-2 or really any virus if I can avoid it. Well, they either respect me, or they know they don’t want to start a conversation with me about it that will end a long email containing a list of peer reviewed publications and a few extra reasons they should be more cautious themselves. Either way, they are part of my personal risk equation.
Anyone who you regularly come into contact with should be part of your personal risk calculation. Because my contacts are thoughtful and respectful, I am confident that they will let me know if they’re not feeling well so we can reschedule and we do. They don’t mind doing things outdoors and have taken COVID-19 tests when asked too before events. Therefore, even though these precautions are not perfect, they do ultimately reduce the risk of infection and during low-risk periods make me more confident to spend time together without wearing a mask. If you have less understanding people in your life, you may want to adjust your activities and/or mask more often around them if you are indoors.
Always be prepared
Going out for the day and not masking sometimes doesn’t mean I’m unmasked the whole time, situations may change and I really might want a mask on. For example, I might have an off-peak lunch in an uncrowded space with another COVID-19 conscious friend next to an open door but then head to a packed grocery store where I hear a few people coughing. Maybe I’m traveling between home and some meetings with just a few people using public transport, during which I will mask for the trip. Another example is when I finish giving a talk on a stage but then have to walk through a crowd that is going to a wedding reception in the same hotel, I’ll quickly put on a mask until I am back outside. Therefore, I always have a couple of masks with me and keep a couple spare masks in my car.
Summary
Here are a few examples that I would consider low, medium, and high risk for SARS-CoV-2, how they could change.
low risk: An outdoor hike on trail that isn’t crowded and provides plenty of space to walk around other people. This would become a higher risk situation if the people you’re hiking with are actively sick, there’s a new variant on the rise, and of course if you shared a car ride over with them. But if you pass someone on the trail who is sick and they do not cough on you, it still remains a very low risk situation.
intermediate risk: High ventilation, moderately crowded space with intermediate waste water levels of SARS-CoV-2. Depending on the activity and how crowded my immediate area is, and how long I plan on spending there, I may or may not choose to mask. But, if you changed the amount of ventilation, making it a low ventilation, moderately crowded space, with intermediate levels of wastewater virus detection, I would choose to mask, as I did at a recent concert in Chicago. If I do choose to not wear a mask in what I consider an intermediate risk situation, I am always on the lookout for reasons to pop the mask on. For example, four days into a recent international conference I attended (and did not get sick) a woman a row behind me started shaking everyone’s hand around her explaining how she introduces herself to everyone one seat away, then she started actively coughing - I didn’t shake her hand, my mask went on.
high risk: A packed indoor venue with poor air circulation, or for example, a choir concert, gym, or restaurant that is packed full of people while a new variant is actively spreading and local wastewater levels are rising. Here proximity and activities matter. For example, not everyone in the restaurant will become sick, and during a choir concert the audience will have a much lower chance of getting sick, while people close to the sick person singing will have a higher likelihood of becoming sick.
Vaccination and Immune Experienced Populations
As a virus moves from a pandemic emergency phase into an endemic phase infection patterns become more well established and typically fewer people get sick, debilitated by, or die from the disease. This is because the population has encountered the virus, a vaccine or both, and some level of population based immunity has been established. Even if it is not true ‘herd immunity’ an immune experienced population also has reduced virus spread as some people simply won’t become infected (in a given period of time) and others who do will have lower viral loads. The only potentially confounding factor here is that SARS-CoV-2 does cause immune system dysfunction and dysregulation and for some people rapid re-infection has been documented. I am looking forward to additional research on how this impacts virus mutation dynamics and spread among a population.
That said, SARS-CoV-2 is still an incredibly dangerous virus that I wish had been contained when we had a chance. It will continue to reshape the way we live for generations to come. I still remember the day in early 2021 that I realized we would never achieve herd immunity, and the virus would be with us forever. Unlike other respiratory illnesses, SARS-CoV-2 can attack the vascular system of the body, impacting every organ and physiologic function from heart, to brain, to liver to an unborn child. This is why it is so important for people with additional health risks and people who are pregnant to practice good personal safety when it comes to this virus, and request that their family members do as well. Infection with SARS-CoV-2 can also trigger the development of secondary disease and/or Long-COVID at higher rates than other viruses we have in circulation. It is likely as research continues we will uncover additional disease development directly associated with SARS-CoV-2, some diseases take longer than others to develop.
Therefore, although fewer people are getting sick and dying from COVID-19 I still choose to mask on a regular basis. This is also why I spend time analyzing patterns of infection, disease spread, and new variant development. The best way to avoid secondary complications is to prevent infection to start with.
Presymptomatic v. Asymptomatic Virus Spread
I have often seen people confusing presymptomatic and asymptomatic spread of viruses in comments on my posts. Presymptomatic spread is something that happens with nearly all viruses where there is a period before someone exhibits symptoms, but the viral load in their body is high enough that they can begin to spread the illness. Measles for example has a very long presymptomatic spreading period, at least 4 days prior to onset of a rash. Influenza can spread presymptomatically for about 24 hours before someone begins to have symptoms. SARS-CoV-2 can spread for 1-2 days before symptom onset in the rare case up to 4-6 though these numbers were typically seen earlier in the emergency phase of the pandemic. There are of course exceptions to each of these but in general, symptomatic spread of a virus is when most people become ill from contact. In certain situational studies presymptomatic transmission was dominant for SARS-CoV-2, however this seemed to be driven by special circumstances such as close, prolonged contact and/or early variants that had a increase in contagiousness and immune evasion, such as the Delta variant. As virus infection rates have reduced with current variants, more research defining the rates of presymptomatic, asymptomatic, and symptomatic disease spread would help people, as well as institutions better assess true risk. A modeling study that reviewed 130 publications in 2022 found that presymptomatic transmission in households (close contact) could be a major driver of infection, but that asymptomatic infection (never developing symptoms) had a significantly lower rate of infectivity. Another confounding factor in the attempt to understand presymptomatic v. asymptomatic transmission is that not every study performs complete follow-up, in this study about half of the subjects initially classified as asymptomatic cases went on to develop symptoms and were in fact ‘presymptomatic.’
In general, people who do not develop symptoms during viral infection (and they have functional immune systems) have lower viral loads. Asymptomatic infection can occur for many viruses, including those we are vaccinated against. Some people, for example, can have asymptomatic measles infections, but do not, based on our current understanding, have any adverse events though they can spread the virus - but at lower rates. The reason for lower rates of asymptomatic spread is that when the virus is well controlled by an immune response (so you don’t have symptoms) in most cases this means that the person has a lower viral load. During early cases of SARS-CoV-2 this may have not been the case due to how new the virus was and these dynamics are likely now significantly different given that the global population has now encountered several variants of the virus via infection, vaccination, or both. Regardless, even a vaccine inexperienced population of people showed in a 2021 study that household (close, constant contact) rates of SARS-CoV-2 transmission from asymptomatic people were significantly lower than that of people who were presymptomatic or symptomatic. For asymptomatic secondary attack rate (how many people got sick from an asymptomatic household member) the researchers found that it was about 1.8% in China among a vaccine and virus inexperienced population, and 2.2% in other countries. A more recent, though smaller study published in 2024 found that asymptomatic children followed from January 2021 to April 2022 infected household members at lower rates than presymptomatic household members.
Though there is evidence presented in some studies that household transmission rates from children may be similar, the numbers are highly variable. It is important to remember that these studies were done with prior variants and often vaccination naive populations where even an asymptomatic infection (likely driven by a combination of genetic factors) would likely have higher rates of viral load simply due to immune system inexperience. As viruses become endemic spreading rates are reduced due to an immune-experienced population generally carrying a lower viral load, which reduces the likelihood of spread.
Because it is impossible to tell who is asymptomatic, presymptomatic, or even symptomatic with a heavy dose of cold medicine on board, I tend to rely on wastewater numbers for my assessment of what is generally going on in the population around me. As always active symptoms are a good reason to take a step back, put on a mask, and/or leave if you don’t want to risk getting sick.

Places Where I Think More Masking Should Happen
If more people were self-aware and conscious of how deadly diseases can spread, we’d have fewer risks and lower overall viral infections to contend with. It would be fantastic if we lived in a society that allowed for more sick leave, had free vaccination programs, ready access to inexpensive healthcare, and people put on masks as soon as they felt a throat tickle. We’d have far fewer needless deaths and disability from viral infections. However that simply isn’t reality. If I only had two places where I could implement change, I believe that schools and doctors offices/hospitals would be a great start to reducing the spread of infectious disease.
Schools and daycares are places where viruses spread readily. Every year when children go back to school after the summer viral illness spikes across the entire United States population as a result. This is not a new pattern, it was documented before the SARS-CoV-2 pandemic. Now SARS-CoV-2 is one of those viruses that begins to spread more at the beginning of the school year. Viral spread in schools can be reduced in a few ways. 1. Updated ventilation and filtration, 2. Improved handwashing protocols and cleaning protocols, 3. Improved vaccine uptake requirements. But there has to be political and parental will to push initiatives like this forward.
It would also be highly beneficial if we could reduce the number of children being sent to school sick, however, the lack of at-home child care in a world where parents often must work doesn’t allow for this to be a reality in our society today. If children are sent to school sick and or would like to avoid illness at the beginning of the school year removing the stigma around mask wearing during this time would be incredibly helpful for reducing disease spread.
Another place where masking can make a huge difference is with doctors and nurses who work with vulnerable patients. I routinely hear from patients who are uncomfortable when their doctors and other caregivers who fail to wear a mask around them. This should be a wake-up call to doctors and medical administrators.
Patient trust is at an all-time low. And while we do find ourselves in difficult times to navigate (some patients may be upset when a doctor wears a mask), there are ways to make your patients feel heard and comfortable in your care. A simple solution could be giving your patients a box to check if they prefer for you to be masked when they visit. If everyone at your chemotherapy infusion center is asking for this option, it could signal an important step towards building the doctor-patient trust relationship back. Care centers that serve chronically immunocompromised people should consider offering masks to everyone who enters. I personally have requested that my dentist and hygienist be masked for every visit, but some people may feel more shy and not self-confident enough to advocate for themselves given the polarization around the topic. Small changes can help re-establish trust and protect people.
Summary
I sincerely hope that this insight into how I approach my own personal infection risk is helpful for you and your loved ones as you think about how to best protect yourselves from infectious diseases going forward. Remember that everyone should take into account their own personal health history when assessing personal risk and if you have any specific questions, they are best discussed with your own doctor.
How do you handle the possibility of presymptomatic spread? That’s my primary concern and the reason I haven’t let my guard down
Thanks so much for sharing your personal protocol and the data backing up your choices.
I really think if we ever get out of science denialism (before the next pandemic), a good public health message will be something like, “take one with you.” I mean just have a couple of masks in your car or purse or whatever. If you find yourself in a higher risk situation, put one on.
Instead, Americans are so attached to binary thinking, they can’t conceive of masks as a health tool like an inhaler - just have one with you even when viruses aren’t running rampant.
I too am still Novid, in large part because of your early guidance and developing those strategies into routines.
As I have CVID, I mask where I’ve always masked—drs offices, crowded stores—high transmission areas. But I too have also relaxed my mask wearing for quick in-and-out stops and small stores, at drive-thrus (yes I was one of those), and with friends who don’t show signs of illness.
But the two thresholds I will not cross — for the REST OF MY LIFE — unmasked are:
Public transportation (including air travel)
And
ANY PUBLIC RESTROOM. (This one I think has been key in keeping me Novid.). E.g., If I eat unmasked at a restaurant and do have to use the restroom, I always put a mask on as I head toward the restroom.
Again thank you for your early and frequent guidance that has helped keep my family safe and limited infections in our family of five to just 3 instances: 0 for my husband; 0 for me; 1 for son in law; 0 for nephew; and 2 for daughter who also has CVID.
Being vaccinated at least once a year (I have been every 6 months until this year), the use of PAXLOVID when our daughter did contract covid, and adaptive mask wearing have all lessened our risk of infection, and severity for the 3 cases we have had “in-house” since 2020.
To your guidance, I added my own personal rule: NEVER use a restroom away from home w/o a mask!
Thank you for all you do for us!!!
(Also: hi Dr Rubin!)