


Introduction to Long COVID: Diagnosis, emerging treatments, and future research directions
Part 1: Introduction to the LIL_Science Long COVID Series

Introduction
Four years after initial lockdowns we are still tackling the fallout of the first pandemic in 100 years. However, unlike influenza which can also have lingering physical effects, it has become clear that SARS-CoV-2 causes life-long physical damage for a high number of people.
The management of post-acute sequelae of COVID-19 (PASC), also known as Long COVID is an area of rapid development. Long COVID is an umbrella term encompassing over 100 symptoms that are causally linked to COVID-19 infection. This can be extremely frustrating for suffers of Long COVID as well as Physicians looking for ways to help their patients. The goal of this multi-part series is to summarize where we are in approaching the set of diseases that can be triggered by SARS-CoV-2. The goal of this series is to summarize what has been learned about Long COVID to date, where we stand four years after the first lockdowns, the future of Long COVID treatment, and cutting edge research.
Since early 2020 I have followed the development of the knowledge base surrounding Long COVID and the scientific advances towards understanding the etiology of the variety of symptoms. I have been waiting for the right time to write this series, knowing that good science and advances in medical care often take time to be tested and developed. I believe the time is now. Even though the collective ‘we’ is still in the process of defining and learning more about Long COVID many people are suffering without answers, summarizing what is known currently will be helpful to many.
Long COVID is especially difficult to tackle because of they myriad of presentations where some patients may have only temporary loss of taste and smell, others may have multi-organ involvement. Now in early 2024 we are at a point where we are beginning to understand the direction Long COVID caused diseases are headed and we are closer to classifications that will assist in defining best medical practice.
It is my greatest hope that this series will be quickly ‘dated’ in terms of the information provided. If that happens it means the science, medicine, and solutions for people are rapidly advancing.
Where Are We Four Years After Lockdowns?
COVID-19 Deaths Have Been Significantly Undercounted
Four years after the United States went into lockdown to reduce the spread of the SARS-CoV-2 virus we are still grappling with the impact of the first global Pandemic in 100 years. In four years the United States has lost an estimated 1.12-1.18M people to COVID-19, more than the World War I, World War II, The Korean War, Vietnam, and Afghanistan wars combined. Studies have reported that the COVID-19 death toll in the United States was underestimated by between 17% and 36% (References 1, 2, and 3).
Deaths per 100,000 in the United States through 2023 had the highest death rates in the indigenous community. However, this study demonstrated that the proportion of excess deaths not counted as COVID-19 deaths was higher in counties with lower average socioeconomic status. The same communities that have been shown have the highest death rates.

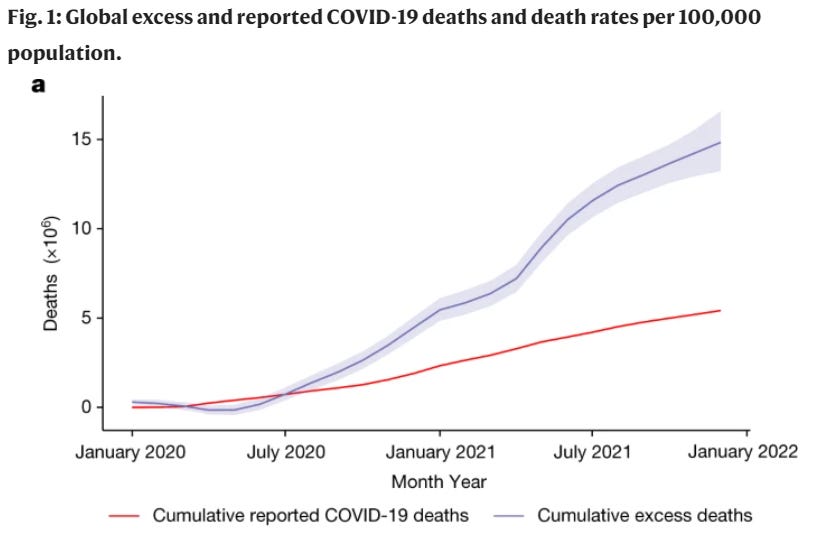
Globally, the WHO estimates excess deaths for the years 2020 and 2021 were an average of 2.74-fold more deaths or 14.83 million excess deaths globally more than the 5.42 million reported as being caused by COVID-19. The largest underestimate of deaths were seen in India though a significant undercount in deaths was seen globally.
The staggering death count from COVID-19 does not include post-infection deaths that may be due to disease or events triggered by recent SARS-CoV-2 infection, or Long COVID. It is possible that much of the excess death was due to SARS-CoV-2 infection and the post-COVID-19 health issues that ensue for many.
While vaccination and antiviral medications have significantly reduced acute COVID-19 deaths, COVID-19 is still fourth leading cause of death in the United States. SARS-CoV-2 is the only virus in the top 10 causes of death, as of this writing, it is the 4th leading cause of death after Heart Disease (1st), Cancer (2nd), and Accidental Death (3rd).
SARS-CoV-2 infections are significantly undercounted in the United States
As of March 2024 the CDC is estimating about 110 million documented COVID-19 cases. However, seroprevalence testing for Sars-CoV-2 infection indicates 77.5% of people in the United States or about 256 million people were already been infected by October - December of 2022. Indicating there are at least double the number of infections as what is officially counted.
It is also difficult to determine the number of repeat infections. Seroprevalence data indicates that in 2022 the population went from 48% having been infected with SARS-CoV-2 to 77.5% indicating a ~ 30% gain in new infections across the United States population in 2022.
What happened in 2022 that allowed for 30% of the US population ~100M people to be infected with SARS-CoV-2 when they have previously avoided it?
As virus variants mutate the more infectious variants tend to outcompete previous variants. There as been a steady increase in how infectious SARS-CoV-2 variants are while there has also been an expansion of mutations enabling immune system escape. Virus evolution paired with how infection management has evolved or been eliminated has contributed to increased virus spread. Here are some of the changes in how SARS-CoV-2 was managed in the United States in 2022:
The CDC reduced quarantine times after exposure or infection in January 2022
Mask mandates were lifted nationwide by the CDC and several states in the beginning of the year.
Multiple highly contagious subvariants of Omicron began circulating in tandem.
2022-2023 bivalent booster was not available until just after the start of the school year for children over 12 years old. For age groups under 12 a booster was not approved until October (5-11 yrs old) and December of 2022 (6 mo - 5 yrs).
Bivalent booster approved in Fall of 2022 did not match primary variants in circulation during the 2022-2023 respiratory virus season.
SARS-CoV-2 Continues to Spread
COVID-19 news fatigue, the politicization of science, and an urge for to ‘return to normal’ have swung the pendulum of public will away from virus mitigation.
Unmitigated spread and lack of awareness regarding COVID-19 is especially dangerous for millions of immunocompromised Americans and older people whose immune systems are in general less effective at fighting infections. Communication regarding COVID-19 remains poor. Notably, a physician friend over 65 had not yet heard that the CDC and ACIP had approved a second SARS-CoV-2 vaccine for 65 and older for the 2023-24 season. I was the first to inform him, weeks after approval, despite his active medical practice.
COVID-19 can kill younger healthy people or leave them seriously disabled, though this is often downplayed. Few people I encounter know of the case studies of otherwise healthy children under 10 years old having pacemakers placed after COVID-19 infection or the increase in the development of Type 1 Diabetes, a lifelong insulin dependent disease in children after COVD-19. These are only a few of the issues children face with COVID-19 infection and repeat infection.
Unfortunately, basic systemic measures to protect children and adults have not been realized in shared spaces such as schools and many office buildings. Much like buildings in California are required to undergo earthquake retrofitting for safety, upgrading air filtration systems in schools and office buildings would be a strong start in the fight to reduce disease spread. Encouraging people who are actively sick to remain home is readily ignored as a common sense public health measure, as well as simple interventions such as mask wearing.
People who have continued to get update SARS-CoV-2 vaccines have lower hospitalization and death rates. Despite this, vaccine uptake is incredibly low. Vaccination is no longer free, but they are covered by most insurance companies. Some programs exist for low to no-cost vaccination however some people have reported that they find the programs difficult to navigate. Unfortunately people who are insured but insurers fail to cover the COVID-19 vaccine are left paying full price, which for many is unaffordable.
At some point, I expect public will to shift in the other direction. Unfortunately, for many it will be driven by direct experience with SARS-CoV-2 infection and possibly an emergent health care crisis.
How many people in the US have Long COVID?
Estimates vary widely and depend on what is classified as Long COVID and how long after infection people are reporting the symptoms. Four years later, some people have never recovered. Many symptoms are silent such as some heart disease, kidney, and liver damage. Assuming 77.5% infections across the US, not accounting for repeat infections which can increase the chances of developing Long COVID, as many as 25.7 million Americans had experienced or are continuing to suffer from Long COVID by 2022. KFF data shows that in January 2023, 11% of people who have had COVID are still suffering from Long COVID, which is approximately 28.2 million people. Although we do not have the data for the whole year of 2023, it will be important to understand if these numbers are continuing to grow.
Assuming up to at least 28 million Americans have experienced and/or are continuing to suffer from some form of Long COVID this makes it the fastest growing, second largest morbidity and mortality causing disease category in the United States. This is caused by an airborne respiratory virus and the number of people suffering are just behind heart disease, but nearly double that of the 17M people living with cancer. These numbers are likely an underestimate.
But what is Long COVID and how are we going to treat it?
How is it that we don’t have any clear path forward or rules for tackling the second largest and most rapidly expanding disease category in the United States?
The short answer is that Long COVID is new.
As with any new virus and set of diseases it takes time to investigate and in the case of Long COVID categorize and name the pathologies, and develop treatment protocols.
In 2024, this science and application therein in medical practice is still a very nascent field, but we have come a long way since 2020 but science and medicine are still playing catch-up.
Will There Be A Solution For Long COVID?
Unfortunately, it is unlikely there will be singular solution for treating Long COVID. The wide variety of clinical presentations that fall under the umbrella of PASC will make it necessary for physicians to think collaboratively and across specialties when assessing a patient care plan. With the sheer number of people impacted by this virus specialists in Long COVID care may become necessary.
Finding ways to treat Long COVID is critically important as it is estimated that Long COVID incidence among non-hospitalized adults with COVID-19 ranges from 7.5% to 41%. Although many recover and the number of people reporting having Long COVID is declining, the reported 11% that currently have Long COVID is likely a significant underestimate. Much of the physiologic damage that is caused by COVID may remain silent.

The best way to avoid Long COVID is to not get COVID. However, this has become increasingly difficult as mask mandates have been dropped, COVID isolation periods are increasingly shortened, and vaccines struggle to keep up with the rate of variant development. Those that have managed to completely avoid asymptomatic SARS-CoV-2 infection and development of Long COVID are nearly exclusively vaccinated with updated vaccines, masking, avoiding indoor gatherings, and likely have had a bit of luck, genetic or otherwise.
Similar to how many underestimated the initial impact of SARS-CoV-2, we are likely underestimating how far in the future the long-term impact COVID-19 is from wreaking havoc on a systemic level. In the meantime, scientists and physicians are continuing to research and address the fall-out from this host of new virus caused diseases yet to be individually named and categorized.
In this series, I hope to shed light on current research and medical reports addressing numerous ailments that fall under the umbrella term Long COVID. Over the next few months I will publish here on what is known in the following areas, many of which may overlap:
Inflammatory Responses: Acute and Chronic
Metabolic Impact of Long COVID
Immune System Dysfunction and Dysregulation
Neurological Impacts of Long COVID
Vascular Impact of COVID Infection
Organ Systems: Cardiac Issues Post COVID infection
Organ Systems: Kidney and Liver Damage Post COVID Infection
Organ Systems: Lung Issues Post COVID Infection
Organ Systems: Gastrointestinal
Endocrine System Disruption in Long COVID
Reproductive Health and Long COVID
Long COVID in Children
COVID and Cancer
Miscellaneous research and new directions
Final Thoughts on Long COVID
I’ll begin with Inflammatory Responses to SARS-CoV-2: Acute and Chronic next week.
If you would like to support this series please subscribe for a monthly or annual subscription. Your support helps me continue to make free content for others who may find it helpful.
As always the writing in this series and information shared is not intended to diagnose, treat, recommend treatments, or do anything more than provide scientific education based on peer-reviewed literature. Any opinions shared in this series reflect only the opinions of the author unless otherwise referenced.
Thought I pass this along: https://www.nature.com/articles/s41590-024-01754-8
Iron dysregulation and inflammatory stress erythropoiesis associates with long-term outcome of COVID-19
Hi there,
So, I was a bit curious about your introduction in which you stated that this is the first pandemic in 100 years. Maybe in such a scale but hardly the first one in a hundred years. Granted, the scale is similar but we had a number of pandemics in the 20th century, not to mention this century. https://stacks.cdc.gov/view/cdc/16102