


Onshoring Infectious Disease: Shortsighted Cuts to Health Programs will Lead to Increased Infectious Disease Spread
Disease increases we will see in the United States in the coming months to years.

Introduction
Infectious respiratory diseases can spread very quickly. In the last five years I have not been on a single plane flight (well over 50 flights) without having at least one person with a persistent, hacking, cough sitting within a few seats of me.
I have not gotten sick from travel since consistently wearing a well-fitting N95 from terminal door to outside the baggage claim. As I wrote the first draft of this post on a flight in February of 2025, a woman next to me asked if I had an extra mask because the person in front of us has been coughing so violently her nose started to bleed and she ran to the restroom holding it and still coughing. The woman next to me wore one of my signature navy blue KN95s, I hoped the best for her. It’s always best to wear one from airport entry to exit.
As I wrote the first draft of this post in early February during the dismantling of USAID which may have had something to do with it’s internal audit of payments made to Starlink. USAID accounts for a small portion (0.3%) of the United States (US) budget, but is arguably a net positive in terms of international relations and stability as well as reduction of life-long debilitating disease both in the United States and abroad.
This article detailing USAID impact was published in Science on February 28th, 2025 “‘A bloodbath’: HIV field is reeling after billions in U.S. funding are axed”. In summary, millions of people will be directly impacted with a near immediate shift in resources to reduce the spread of HIV/AIDS.
I can hear echoes of push-back regarding ‘put America First’ and ‘why do we support health programs in other countries’?
Simply put, diseases do not respect borders and it is far less expensive to control, treat, and work towards the elimination of a disease overseas than it is to manage an outbreak in the United States.
As I brush-up this draft for final publication the US stock market is set to open at even lower levels than yesterday (April 3rd) which had already wiped close to $3 T of capital out of the market. I will also remind the single issue voters focused on the economy that economic health and population health are tightly linked. In my opinion, the adoption of AI only partially decouples this longstanding fact, though others may quietly believe differently.
To summarize the breakneck speed of public health dismantling both at home and abroad made it impossible as I sat on a plane in early February trying to assess the far-reaching implications of agency dismantling on public health. I waited, and watched the dismembering of long-standing agencies this week as highly experienced world-renown experts were fired or resigned.
I am glad I waited. In February the chaotic operations of this administration had only just begun, and although we are not sure today if they have ended, I believe the trajectory is now clear. For example, grant funding awarded to states to support tracking, prevention and control of infectious disease was canceled April 1st, though the cuts were temporarily blocked by a federal judge the funds may be in limbo while several states move to sue the administration. Chaos is par for the course with the current administration, but unlike version 1.0, version 2.0 seems to have intentionally become more tight-lipped (unless you have the signal app on your phone), far less communicative around activities and intentions.
This approach is the antithesis of how good public health operates, this is how you kill people.
Although the dust still hasn’t settled, I do believe we’re in a place where I can describe a few forward looking scenarios that will help people prepare for what’s to come.
Disease Incidence Will Increase: Dismantling of Public Health Programs at Home and Abroad
The US has drastically altered it’s approach to combating infectious disease, research and development, and promotion of educational resources that improve long-term health and wellness. This will have near-immediate impacts on the health and wellness of both US citizens and health around the world.
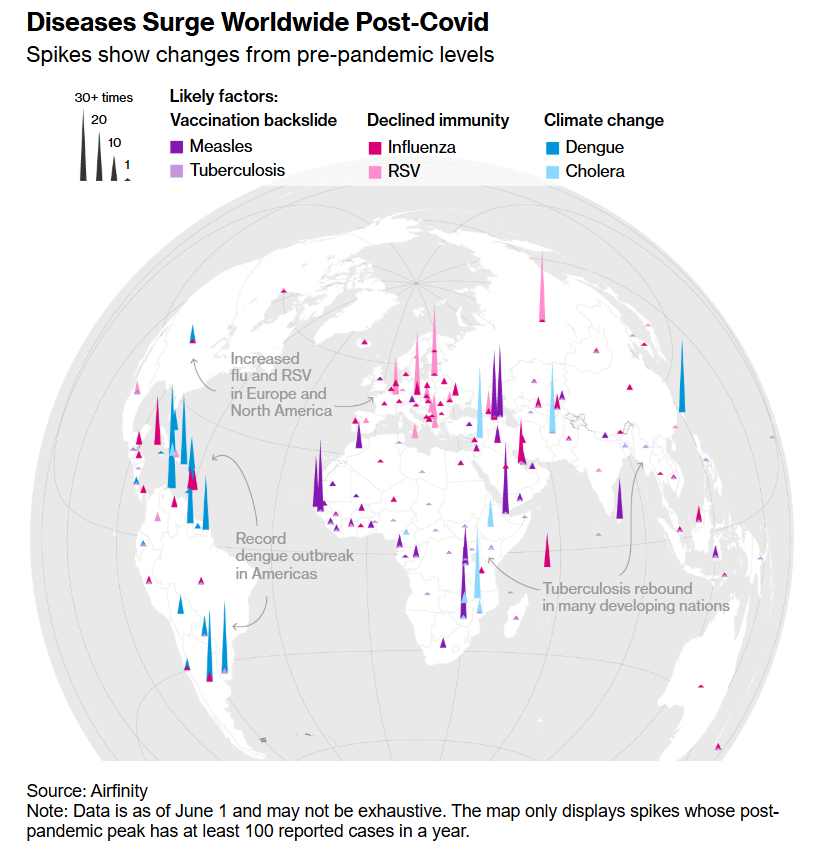
Infectious disease outbreaks were rising before reduction in public health measures. Below is a graphic from “Global surge in infectious diseases as over 40 countries report outbreaks 10-fold over pre-pandemic levels” posted in 2024 by the infectious disease tracking company Airfinity that specializes in independent disease forecasting and health intelligence.

In June of 2024 Bloomberg also published “Yes, Everyone Really Is Sick a Lot More Often After Covid” using the same analysis to highlight 13 infectious diseases that are surging above pre-pandemic levels with some cases surging over 30-fold higher in certain areas.
Many of these diseases have begun to increase in the US. For example, measles, which spreads rapidly in unvaccinated populations and has surged in a West Texas community. This outbreak has lead to over 480 cases, more than all US cases combined for 2024 (285). Texas health officials have indicated it will take months, possibly up to a year to get this outbreak under control.
It is unclear how the West Texas outbreak started, but several other cases around the US have been linked to international travel and exposure to the virus overseas. Regardless of how the outbreak started, it wouldn’t have been possible if MMR vaccination rates were at or above the herd immunity threshold.
On average school aged children in the United States are below the vaccination threshold rate of 95% necessary to maintain population based herd immunity with a significant downward trend starting in 2020.

Reference: “Measles Cases Are Surging—These 6 Charts Reveal Why”, Scientific American.
In addition, all 50 states have communities with exceedingly low vaccination rates which can lead to an increased chance of sustained outbreaks.
Without rapid identification, isolation, treatment, or vaccination programs world wide these diseases which already have smaller outbreaks, will rapidly balloon. Diseases we’ve kept at bay through health programs and vaccination are set to rapidly remerge as a result of reduced vaccination, loss of low-cost pharmaceutical distribution, and disease control measures such as educational outreach and condoms. For example, diseases such as HIV and tuberculosis (many people are carriers) can re-emerge quickly without treatment or access to care.
Below are timing estimates for increased disease incidence in the United States:
HIV/AIDS
Rapid re-emergence of AIDS due to elimination of treatment and prevention programs abroad will contribute to increased disease incidence in the United States. This may be delayed if local programs can swiftly fill the gaps left by the dismantling of USAID, though in many regions this is unlikely. Loss of sex education and prevention program funding both abroad and in the US will increase rate of HIV/AIDS spread. Finally, delayed detection and treatment due to reduction in program funding will increase the rate of spread of HIV/AIDS in the US.
I expect that if we maintain surveillance and reporting which is administered through HHS that we will see an uptick in incidence as soon as 6 months from now with significant spread within the United States population within 12-24 months from now.
Hemorrhagic Fevers (Marburg and Ebola Viruses)
Within the next 12 months I expect there to be an increase in cases in endemic regions and increase sporadic cases outside of endemic regions. I believe that larger outbreaks increase the chances of person to person transmission outside of endemic regions for the foreseeable future.
Areas where Ebola and Marburg virus are endemic has seen increased outbreak cadence over the last couple of years. The last time the United States had an Ebola case was in 2014 with four patients having traveled from Libera and Sierra Leone.
The WHO often sends teams of scientists and medical workers to help identify, contain, and treat outbreaks of hemorrhagic fever, and the loss of US support for WHO activities that help reduce the spread of local outbreaks will lead to larger outbreaks in endemic regions and delays in identification that may delay implementation of travel screening.
Tuberculosis
Rates of tuberculosis infection have been increasing globally (except in in the European Region).
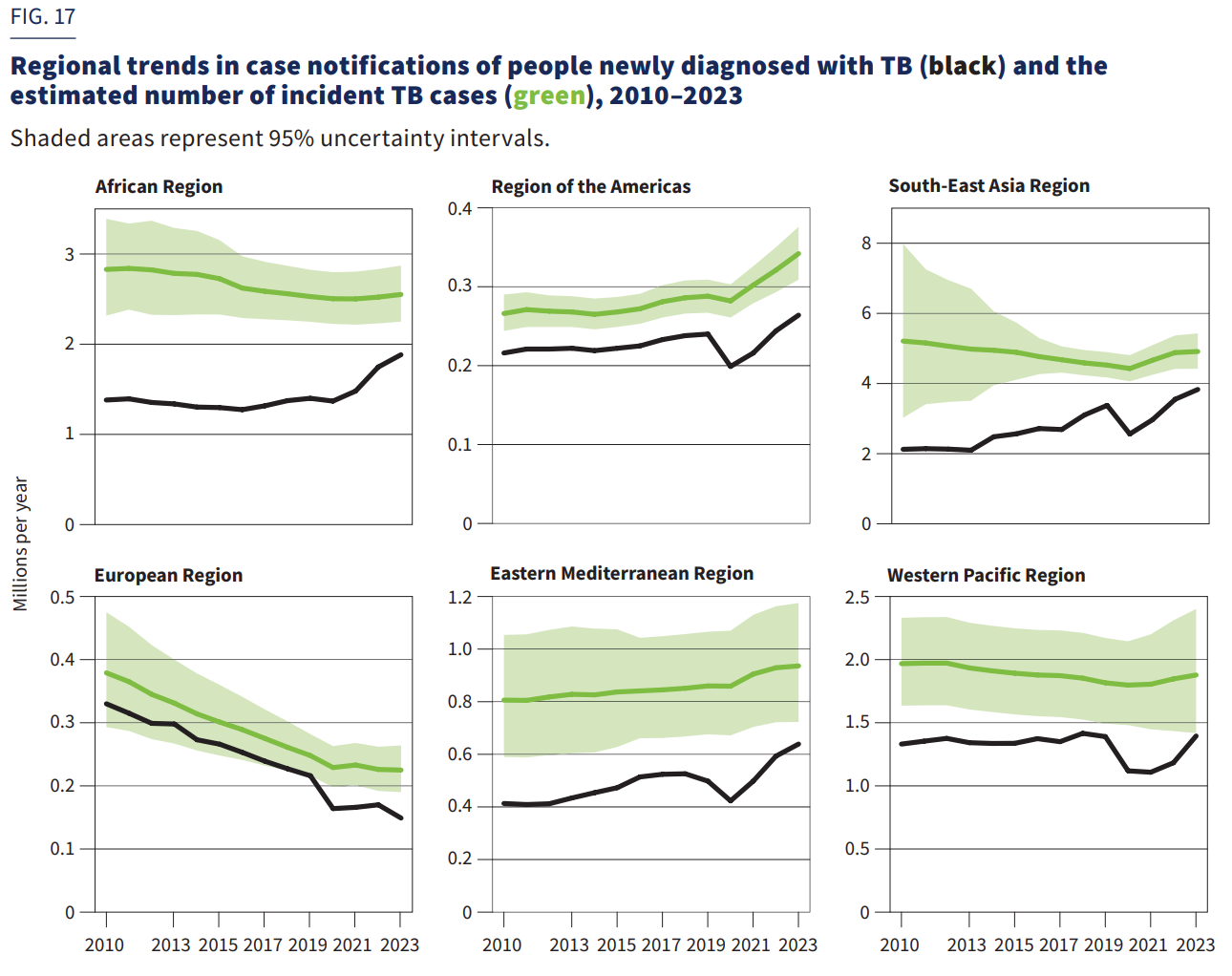
(WHO Global Tuberculosis Report, 2024)
Additionally, death rates from Tuberculosis increased in the United States by >5% between 2015 and 2023.
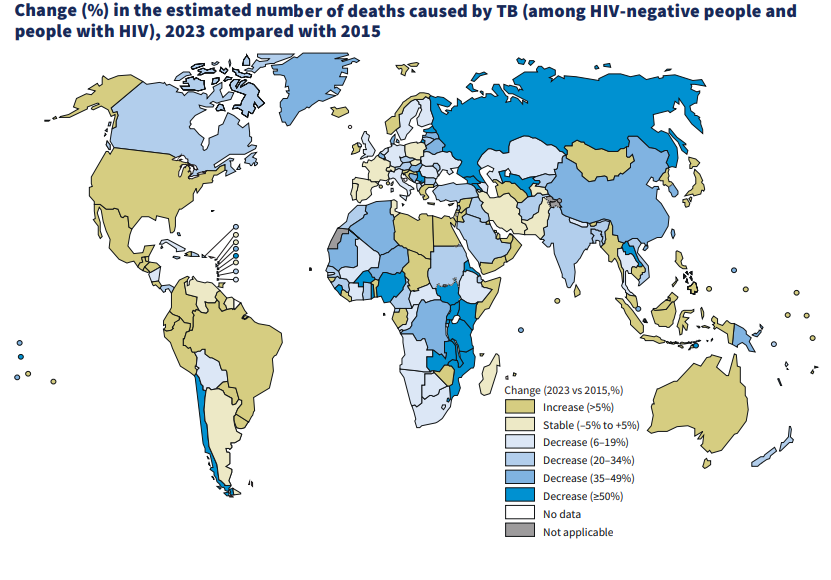
(WHO Global Tuberculosis Report, 2024)
Without continued support of health interventions and testing, I would expect rates of tuberculosis to begin to increase and be detected by health surveillance within the next 1 to 2 years.
Polio
European wastewater surveillance indicates that Polio (though live-attenuated vaccine related) continues to show up in countries that have not recorded a case of Polio for decades. In 2022 the state of New York as well as a few other states embarked on waste water surveillance after a 20 year old Rockland County, (NY) man was paralyzed by the virus.
The United States vaccination rate against polio has continued to decrease in recent years. In some states the polio vaccine coverage was in the 80% range for incoming kindergartners in 2020-21.
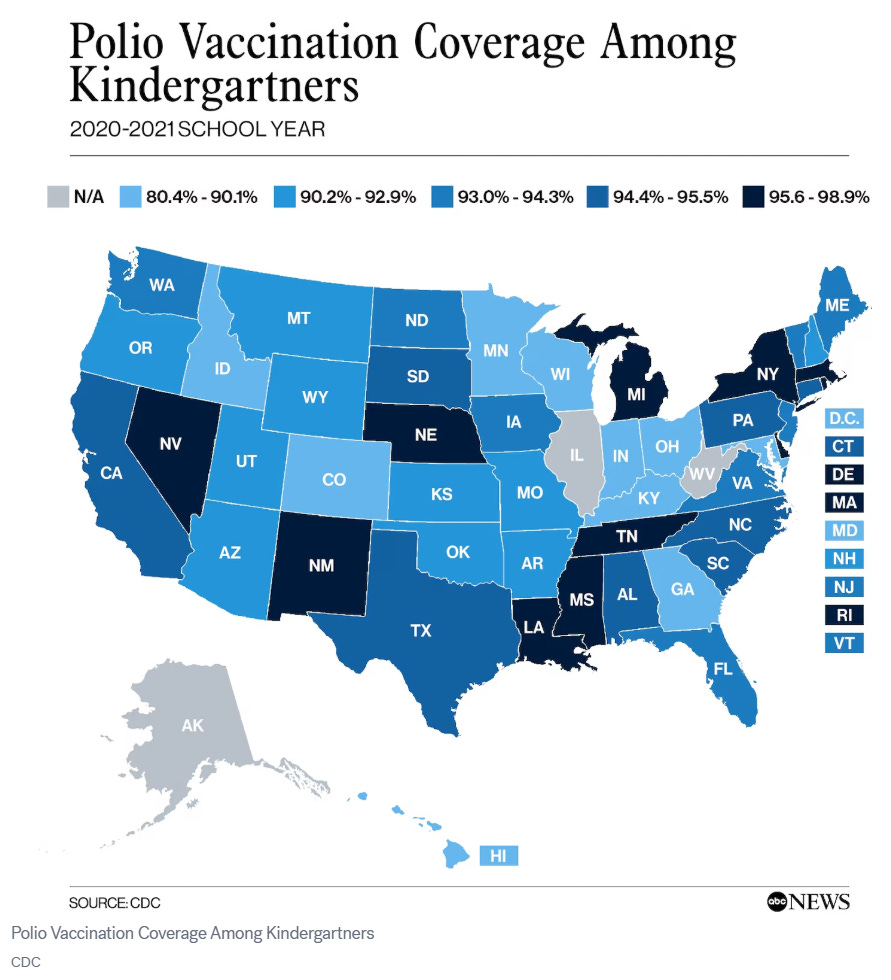
This trend has not reversed with the lifting of pandemic measures with an overall increase in requests for vaccine exemptions and a continued decrease in polio vaccination rates among school-aged children. The decrease in polio vaccination from a US average of 95.3% in 2011-12 to 92.6% in 2023-24 follows the overall trend of decreasing childhood vaccination rates.
Link to this interactive tool and more school-aged childhood vaccination facts can be found here: CDC SchoolVaxView
Unvaccinated children are not protected from polio infection and the sudden USAID and CDC halting of support of global Polio eradication efforts in February 2025 are likely to increase global and eventually US incidence of polio infection.
I estimate that we will continue to see sporadic cases of polio in summer months in low vaccination rate communities with large outbreak potential if vaccination rates continue to drop. The oral polio vaccines was phased out in the US in the late 90s and has not been used since 2000. IPV (inactivated polio vaccine) has been used since the year 2000, however there is no data on how long this vaccine remains effective. Given the unknown duration of modern polio vaccines surveillance is critically important to maintain eradication of polio in the United States.
Measles/Mumps/Rubella
The West Texas outbreak is discussed above, however there have already been several smaller outbreaks around the US as of April 4th 2025. Due to an increase in global incidence and continued decline in childhood vaccination in the US, there is likely to be continuation of sustained outbreaks over the next one to two years with increasing frequency unless vaccination rates are increased. Cases of Rubella and Mumps which can be deadly, have also increased in recent years as MMR vaccination rates have declined.
The temperature of social media responses to the current West Texas measles outbreak are wildly polarized. A significant number of people in my audience are horrified at the obvious back-slide of public health in the US. But a few people seem to think that a children dying from a vaccine preventable disease is perfectly acceptable.
The “measles is no big deal” narrative is fueled by groups like “Children’s Health Defense” founded by the current US Director of Health and Human Services, RFK, Jr. The Children’s Health Defense promotes fearmongering and health disinformation that is directly counter to the global communities standard of care and medical practice. It is important to understand that the professionally crafted narrative of “Children’s Health Defense” are not only counter to standard of medical care in the United States, but their recommendations run counter to medical care and decades of scientific research in all developed nations, without exception.
Out of curiosity I went to their scientific evidence page for vaccines. I looked up the first author of the first study of their study collection. The MD practiced homeopathy and had his offices raided by the FDA because he was charged with giving unproven and potentially dangerous therapies to autistic children after telling the parents he could ‘cure’ them. As RFK Jr. took over leadership of HHS he refused to recuse himself of financially benefiting from lawsuits attacking long-standing vaccines give world wide.
Respiratory Viruses
Elevated levels of respiratory virus infection will likely continue for the foreseeable future. Real-world evidence has finally refuted the ill-advised concept of Immunity Debt that was espoused by celebrity doctors and repeated by ill-advised news media in an attempt to explain surging rates of respiratory virus illness among children immediately after the height of the SARS-CoV-2 pandemic.
This was at best blind ignorance as the evidence against ‘Immunity Debt’ was clear from the country of Sweden that did not lockdown (had a several-fold more COVID-19 deaths than neighboring countries) and had an increase in respiratory virus infections that matched the rest of the world.
One potential cause for the surge in respiratory virus infection that is supported by evidence is that SARS-CoV-2 causes significant immunosuppression post-infection. Immunosuppression appears to last for different amounts of time for different people and the severity may be linked to the severity of SARS-CoV-2 infection. This hypothesis remains to be further tested but mechanistically it is sound. I anticipate this research is forthcoming.
In addition, respiratory virus illnesses, including highly pathogenic influenzas (sporadic occurrences globally), are on the verge of mutation that would enable person-to-person spread. Highly pathogenic H5N1 is one amino acid change away from sustaining person-to-person spread. A single amino acid change similar to the one identified by scientists as supporting person-to-person spread was sequenced from a teenager hospitalized for over two months with H5N1 in Vancouver, Canada. Because there were a mix of variants in the teenager it is possible that the H5N1 mutation arose spontaneously as an adaptation during infection. This indicates that this mutation can easily occur in an infected individual that is immunocompetent. In laymen’s terms sustained person-to-person spread of highly pathogenic H5N1 is imminent.
Early detection and isolation through surveillance, and prevention of spread with influenza vaccines are critical interventions for heading off the next influenza pandemic. Few people continue to wear masks post-COVID and practice regular hand hygiene, but those that do will significantly reduce their chances of influenza infection.
While European countries have begun to stockpile H5N1 vaccines, the Trump administration is considering cutting funding to an mRNA based H5N1 vaccine development program, has fired staff working on the H5N1 response, and has not indicated that any new orders of the currently approved H5N1 vaccines are being added to our stockpile that would cover less than 1% of the US population.
While our population may have some pre-existing immunity to the N1 portion of H5N1 that will help minimize the impact of a pandemic. Highly pathogenic H5N9 and H7N9 have recently been reported in domestic bird populations indicating these potentially pandemic causing viruses are spreading well. The global population does not have pre-existing immunity to either of these influenza strains and I am unaware of any approved vaccine or national stockpile that covers them.
Vector-Borne Disease
Finally, a myriad of parasitic and vector-borne (tick and mosquito) illnesses are being reported further north every year. Here are a few examples:
In the United States:
Alpha-gal syndrome (Lone Star tick).
Rocky Mountain spotted fever (Rocky Mountain wood tick)
Dengue fever (Bone break fever, mosquito)
Eastern Equine Encephalitis (EEE, mosquito)
Without investment in mitigation measures, outbreak tracking, and containment it is expected that these diseases will continue to spread northward and impact new populations.
Why is This Going to Get Worse?
This week HHS underwent a chaotic and poorly-communicated ~25% reduction of it’s workforce. The current cuts to the HHS reduce employee numbers to levels not seen since the Clinton administration, over 30 years ago. The mass attrition also includes several high-level forced resignations or firings of expert scientists and physicians with decades of experience that is difficult to replicate. It is unclear how well the agency will operate going forward even after a period of reorganization.
Rapid dismantling of health program funding both at home and abroad destroys our ‘eyes and ears’ that enable us to identify and try to stop the next pandemic. For example the CDC is a centralized research center for pathogen identification and testing, but has experienced deep cuts firing dozens of people nicknamed ‘disease detectors’ who assisted public health departments with testing and surveillance.
During the prior Trump administration the CDC’s pandemic response team was dismantled mere months before the first report of the SARS-CoV-2 virus. The CDC’s pandemic response team plays an important role in pathogen screening (often at points of entry during global outbreaks), identification, containment, and vaccination. Under the Bush Jr. administration the SARS-CoV virus (the first one) was contained and eliminated by action of the WHO locally in China, and though coordination between the WHO and the US CDC whose actions were streamlined by HHS. Despite the virus having a similar Ro (spreading rate) to the initial SARS-CoV-2 variant. Trump has said he would disband the pandemic response team (again) and it appears that he has made good on that promise in 2025.
The relatively pathogen-free existence of most United States citizens has lulled many of us into forgetting that the fragile bubble of protection we enjoy is directly due to the work of the CDC, WHO, USAID, FDA and many other agencies under the umbrella of HHS.
Funding Cuts That Do Not Significantly Improve US Budgetary Outlook
US agency collaboration with, and support of, the WHO that directs global disease surveillance and programs designed to identify and reduce pathogen spread has ended. Removal of both financial and collaborative support of the WHO will significantly impact these operations. WHO contributions annually, over the last decade were $163 million and $816 million annually, accounting for less than 0.01% of the US federal budget.
Criticism of WHO, especially regarding the early handling of the SARS-CoV-2 pandemic is largely unfounded. The WHO is not a military organization, it relies on cooperation of the nations that it serves and their health care workers and scientists could not enter areas of China that it was not allowed into for treatment and investigation of the SARS-CoV-2 outbreak.
Within the US the narrative that HHS is wasteful organization doesn’t hold up to real-world scrutiny. 70% of HHS spending is mandatory funding programs such as Medicare and Medicaid, while agencies that fund health research and ensure drug safety account for an estimated 11% of the budget. For example, Global Health accounted for 0.1% of federal spending on health programs in 2024, while the FDA tasked with keeping our food and drugs safe accounted for about 0.06% of the total federal budget in 2024.

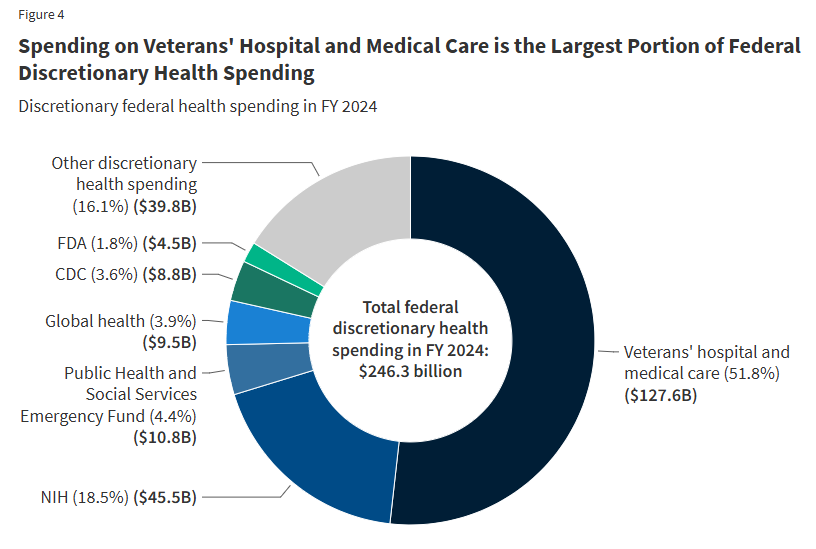
Figure References: KFF Report What Does the Federal Government Spend on Health Care? (2025)
The total 2024 US budget spend was ~ $6.9 T and the NIH accounted for 0.6% of the spending, and much of it is directly reinvested in the US economy. The NIH redistributes taxpayer dollars to fund research in all 50 United States, at a net economic benefit to the state of $2.5 for every $1 granted. Read more about this in the KFF report: “What Does the Federal Government Spend on Health Care?” (2025).
Summary
The rapid and disorganized upheaval of national health programs combined with catastrophic funding cuts has created the perfect environment of defenselessness to increased spread of potentially deadly pathogens. We are under leadership that has no substantive history or vested interest in disease prevention or meaningful public health measures. In fact, the current administrations appointees within the HHS are entirely unqualified and deeply misguided in their approaches to public health. To exclusion, their resumes boast long-standing public promotion of health disinformation and false as well as wildly if not willfully misinterpreted medical information for personal profit.
What Can We Do?
On an individual level you can be proactive in taking control regarding personal health and safety. Both personal behaviors and communicating to loved ones that sexually transmitted illness, vector-borne illness (mosquitos and ticks), and respiratory viruses are potentially on the rise can help reduce illness.
Being prepared can help you and yours stay healthy during these uncertain times. Encourage public representatives to support research as well as health and safety initiatives.
Continue to share well sourced, accurate health and safety information whenever you can. to stand up to the well-funded incessant machine of medical disinformation.
Note: that I have done my best to cover most immediately concerning infectious diseases though this list is not exhaustive. I have left few out, such as clade 1b MPOX which is more deadly and transmissible and may begin to show up more regularly in the US. In general. the loss of vaccine based herd immunity and the disruption of public health measures in the US and abroad is expected to increase global pathogen spread and has reduced the ability of US public health officials to respond to and contain infectious disease outbreaks of known and novel pathogens.
Thank you for your continued support of this research and reporting.
Thank you for this post. I have 3 autoimmune diseases and I’m on 2 immunosuppressants. I wear an N-95 in airports, on planes and in most places people congregate. As you state, things will only get worse. I am not looking forward to this!
Took my MMR titer, born early 60s and had zero immunity against measles! I have immunity against mumps and rubella. I don’t think many people in my age group realize that the vaccine they got in the early 60s was a dead virus and probably not very durable. I did get my booster last week. I definitely see older people in my age group not realizing they are not immune and getting measles at an older age. Thank you for all you do,very scary times.