


On June 15th of 2023 the Vaccines and Related Biological Products Advisory Committee (VRBPAC) part of the US FDA met and discussed vaccine recommendations for the 2023 Fall booster to be produced by Novavax, Moderna, and Pfizer. The full FDA Briefing Document can be found here: Selection of Strain(s) to be Included in the Periodic Updated COVID-19 Vaccines for the 2023-2024 Vaccination Campaign.
At the end of the meeting the committee voted to recommend a monovalent (one antigen or spike protein variant) vaccine based on variants XBB.1.5, XBB.1.1, or XBB.2.3.
All three companies are providing COVID-19 vaccines in the United States are working on a XBB.1.5 variant based vaccine.
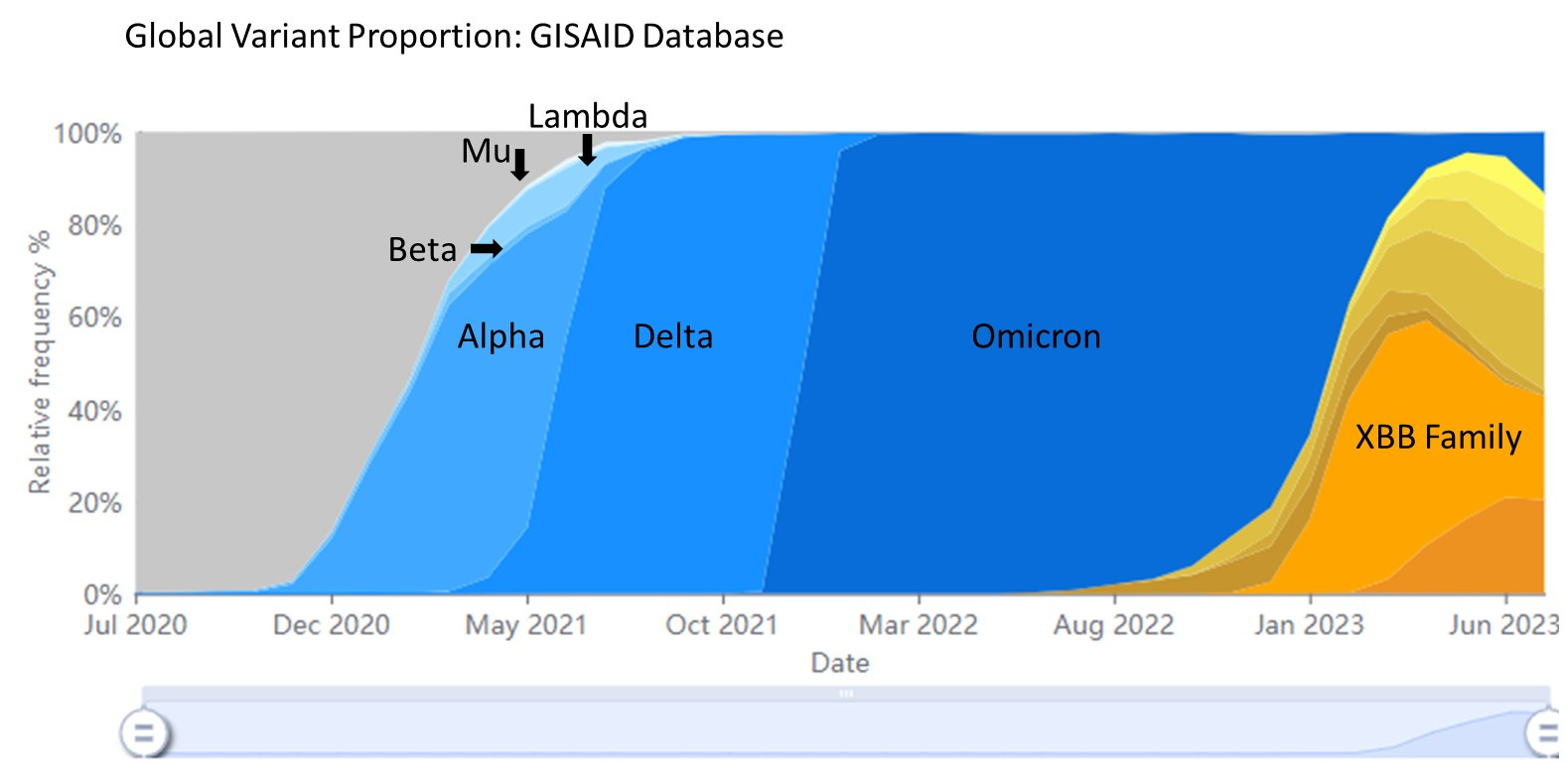
Currently XBB.1.5 is the dominant variant in the US but retreating quickly. There is a mix of variants in circulation per the most recent Genomic Surveillance data from the CDC (below).

Note: Nowcast data is subject to change and variant proportions may be adjusted as more samples collected during a given week are sequenced.
A variant named EG.5 however is showing rapid growth. EG.5 (XBB.1.9.2 with Spike protein mutation F456L - in the receptor binding domain) has demonstrated a significant growth advantage in other countries. EG.5 is most common in China where it was sequenced in April and is now about 15% of sequenced cases.
Currently EG.5 has an estimated growth advantage of 50% per week and is doubling every two weeks. (GitHub Variant report can be found here)
Collectively the variants in circulation around the world are highly mutated relative to the original Wuhan SARS-CoV-2 variant with over 100 mutations in the variants sequenced from around the world. (This data can be found at NextStrain.org)
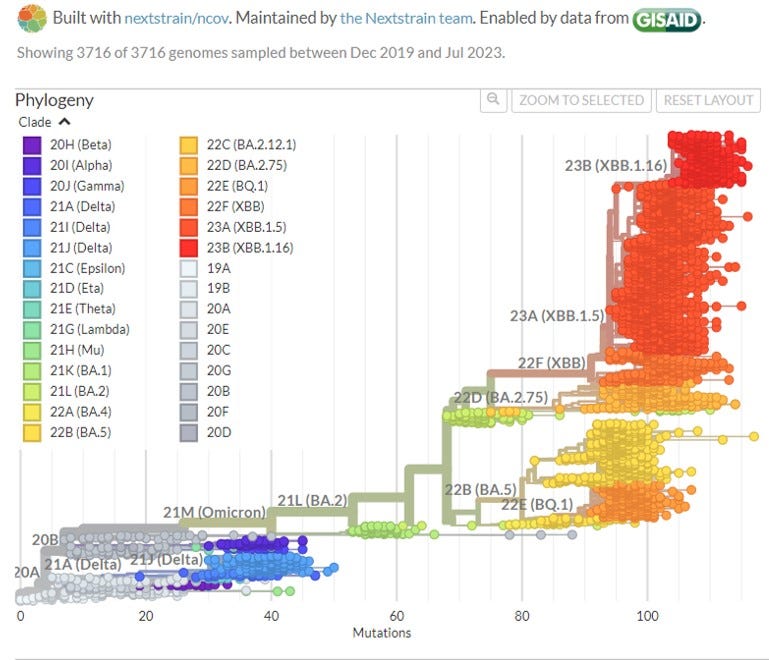
Notably, NextStrain.org shows a small subsampling of known variants deposited in the GISAID database for visual clarity. There are over 5 million sequences submitted to the GISAID database. Unfortunately, global sequence acquisition has fallen significantly from it’s peak in the winter of 2021.
If pharma is developing a vaccine for XBB.1.5 and we have EG.5 on the rise and many other variants in circulation, will vaccine-variant mismatch be a problem this winter?
Surprisingly, as bad as it sounds to be in SARS-CoV-2 Variant soup, I predict the Fall / Winter, baring a wild card variant will not look like prior SARS-CoV-2 waves we have experienced over the last three years. Here’s how I am thinking about this as we approach Fall/Winter 2023-2024.
First, EG.5 and several other XBB family variants do not have a significantly different spike protein from XBB.1.5. In the case of EG.5 + F456L there is one mutation known to confer immune escape, but only partially, it is not expected to cause a significant reduction in vaccine efficacy. The real issue will continue to be vaccine and infection induced immunity waning which will allow for infection but typically a mild course of viral illness. In addition, EG.1 contains the Q52H and Q613H mutations outside of the receptor binding domain of the spike protein. This may have an impact on some antibody binding if antibodies are raised against XBB.1.5, but again, it is not expected to be significant. Other variants such as GL.1 (XAY.1.1.1 + D420N and Y144 deletion) a Delta-Omicron recombinant are derived from prior widely circulated variants and do not contain significant immune escape mutations.
Second, despite the numerous variants in circulation they are relatively closely related to each other or other variants in wide circulation, reinfection is common. However, these variants are closely related enough that a new wave or high infection rate combined with a significant amount of severe disease, is unlikely to be driven by anyone of the major known variants as cross seroprotection and continued booster administration will reduce severe disease in most people.
Third, The natural seroprotection (antibodies) and memory T cells in our population and reduced diversity between variants indicates a reduced likelihood of development of a home-grown variant in the human population. Current data indicates that in the US population we may be nearing virus evolutionary stasis wherein multiple closely related but highly evolved variants remain in co-circulation and infecting people at a steady state. It’s not quite endemicity but it is trending in that direction. Notably it’s not ideal that we are potentially nearing endemicity at the current rates of infection and death, but hospital crippling waves are not likely to be caused by any XBB family variant.
Why this is still bad.
There is evidence that SARS-CoV-2 infection causes immune system dysfunction and dysregulation as well as significant vascular damage, injuring organ systems. In addition, COVID-19 has been linked to neurological issues and in many cases has been found to be persistent in the body for years. We still do not know the long-term implications of persistent SARS-CoV-2 infection, however when other viruses do this we know a host of diseases can emerge as a result (cancers, autoimmune diseases). Despite the variants not ‘feeling’ as significant as prior waves, people can and will continue to become ill from the SARS-CoV-2 virus, increasing the likelihood of cumulative physical damage or extended infection with the virus. This complacency and lack of education or understanding around the long term physical impacts of SARS-CoV-2 will increase the long term disease burden of any population not reducing infection numbers.
In summary, I expect there to be an uptick in SARS-CoV-2 cases and deaths this fall and winter. This, like the notable and significant increase in the spread of other respiratory diseases, will be initiated by the start of the school year in the United States. We will continue to see more new long COVID cases. Unless we have a variant that is significantly different from the XBB family of variants I do not expect a severe wave of COVID-19. A wild card variant is a possibility and I believe we should still be vigilant in sequencing and tracking the evolution of new variants. I am disappointed by the monovalent vaccine approach, and expect this to be adjusted in the future.
What I do expect alongside the uptick of COVID-19 cases this winter is an increase in severe respiratory diseases. However it is difficult to determine how severe waves of Influenza, RSV, and human metapneumovirus will be this year. COVID-19 is still causing extensive immune system dysfunction and dysregulation that lasts for over a year in some people. However we don’t know how much it is impacting children and what recovery dynamics look like for most people. Scientists are working to better understand and define the long term impacts of COVID infection. However, it is clear that in some people production of key cytokines that fight of viruses and cancer are significantly reduced.
The vaccine based on XBB.1.5 should confer reasonable protection from infection based on our current variant soup. An XBB.1.5 based booster will also reduce the likelihood of hospitalization with severe disease. Reduction of severe disease also reduces the likelihood of developing long COVID and possibly other post-COVID issues. Finally, I do not know if it is planned, however I do hope that Pfizer, Moderna, and Novavax are planning to continue to run clinical trials with new variant vaccines before distribution. I will write more about why I believe this is important shortly. Until then, mask-up, stay safe, and get your booster.
Note from the author: I do not charge for access to my Substack because my goal is to provide free access to valid scientific information and critical opinions to all. However, the amount of time to put these write-ups together is significant and my expertise in the field usually ensures I am paid for my time on projects like this. Signing up for a paid subscription for any amount of time will help support this work.
This is a great summary on the current state of COVID-19. I agree that future waves are unlikely to be as crippling to the healthcare system acutely, but I am concerned about the long term healthcare implications due to Long COVID
LIL, Thank You! Thank You! Thank You! This made me so happy to still get.
I don’t think there was a day of uncertainty where I didn’t flip to see what you were saying. I appreciate you. It made me cry when I knew you would be leaving. It made me cry when I just got this email. To say you held my hand through this pandemic is not enough. Please know so many were/are so grateful for you. I hope you are well & safe. -coachg_1